Inositol is a small molecule structurally similar to glucose and plays a key role in cellular communication. Inositol also plays a part in regulating the activities of several hormones, such as the follicular stimulating hormone and insulin. Researchers speculate that insulin resistance is, at least partially, caused by low inositol availability. And indeed, studies show supplementing with inositol can be highly effective for women with hormonal irregularities often seen in acne.
There are nine types, or forms, of inositol, but for our purposes we are only interested of two:
- Myo-inositol
- D-chiro-inositol
Inositol is one of the most promising supplements for hormonal-type acne. While only one or two studies have looked at how it affects acne, scores of studies have shown inositol to be highly effective in women with polycystic ovary syndrome (PCOS). Supplementing either with myo- or D-chiro-inositol significantly reduces insulin and androgen hormone levels. While most women with acne don’t have PCOS, they can certainly benefit from the insulin and androgen-lowering effects of inositol.
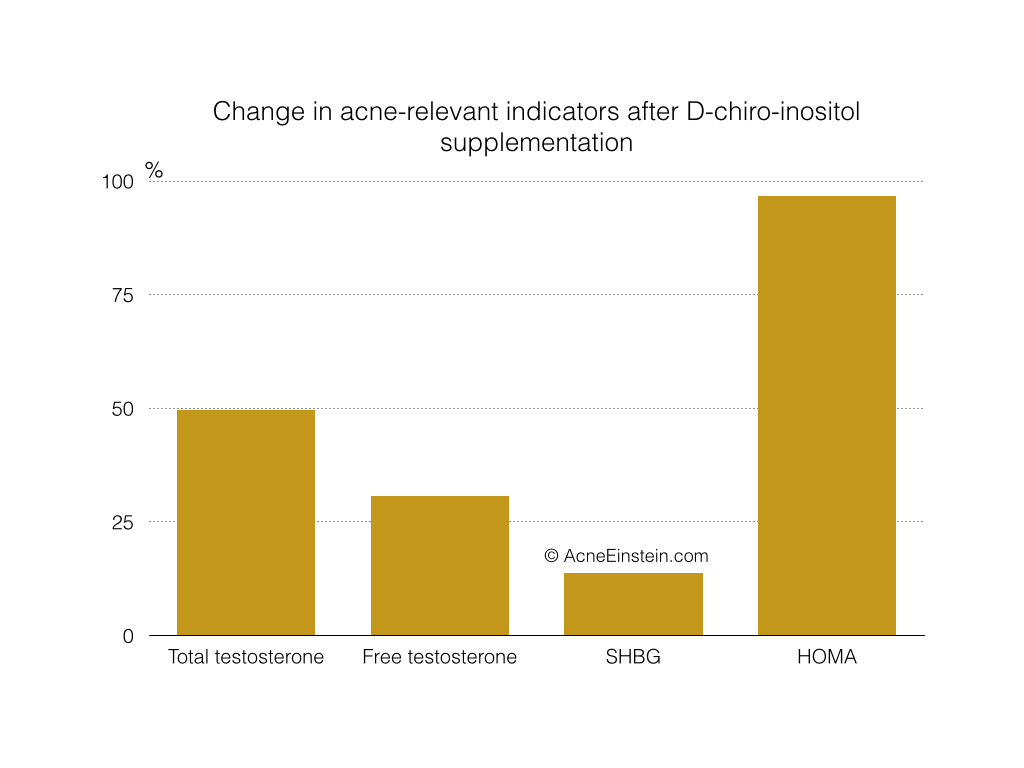
In 2014, Italian researchers published a paper showing the remarkable benefits of D-chiro-inositol supplementation in lean PCOS patients (the group of PCOS patients that resembles female acne patients the most).
In the study, 48 patients were given 1g or D-chiro-inositol and 400mg of folic acid per day for six months. This graph shows the %-change in the acne-relevant parameters.
All of these changes are improvements since the beginning of the study. So for example, testosterone levels dropped and technically the graph should show -49%, but I dropped the minus to make the graph easier to read.
Source: Laganà, A. S., Barbaro, L. & Pizzo, A. Evaluation of ovarian function and metabolic factors in women affected by polycystic ovary syndrome after treatment with D-Chiro-Inositol. Arch. Gynecol. Obstet.(2014). https://www.ncbi.nlm.nih.gov/pubmed/25416201
Let me quickly explain the terms. Free and total testosterone are just that. Most testosterone in the blood is bound to sex hormone binding globulins (SHBG) and not bioavailable. Free testosterone is the bioavailable testosterone. SHBG is especially relevant in acne, and several studies show women with acne have lower levels than women without acne. HOMA is an acronym for Homeostasis Model Assessment and measures insulin resistance. It quantifies how much glucose and insulin combined is in the bloodstream.
It’s hard to overestimate these effects. The effect on insulin resistance is comparable, or even larger, than what several months of regular exercise does for sedentary people.
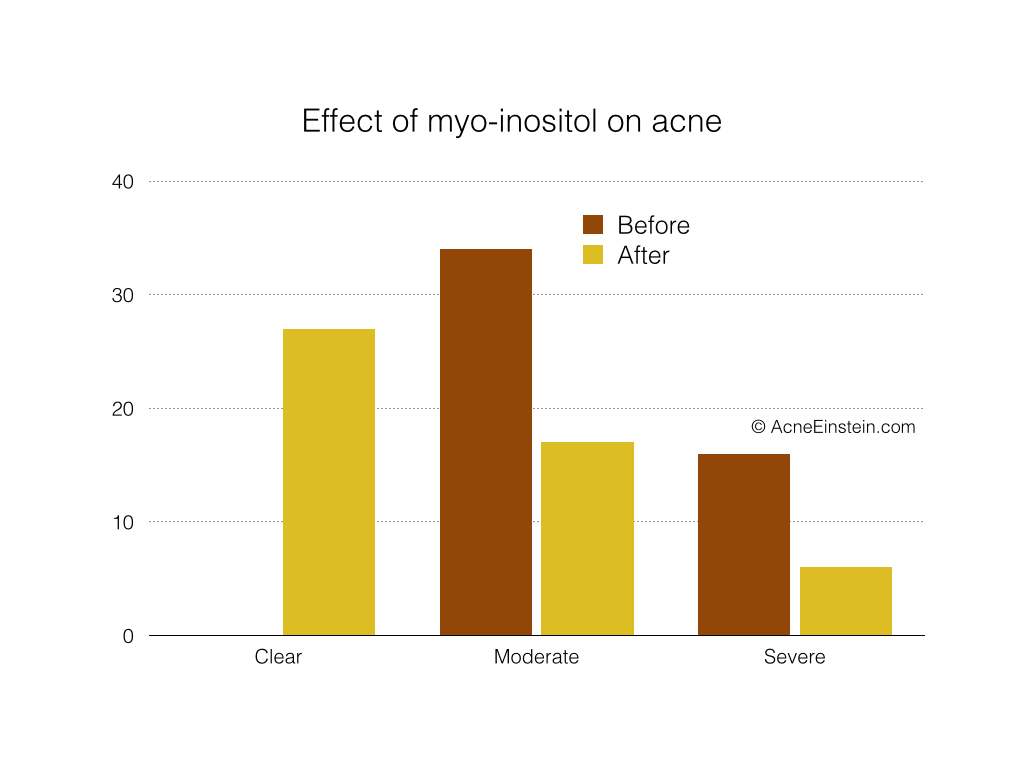
Another study specifically looked at how myo-inositol supplementation affects acne in PCOS patients. The study included 50 women who either had moderate (34 women) or severe (16 women) acne.
This graph shows the effect:
Source: Zacchè, M. M. et al. Efficacy of myo-inositol in the treatment of cutaneous disorders in young women with polycystic ovary syndrome. Gynecol. Endocrinol. 25, 508–13 (2009). https://informahealthcare.com/doi/abs/10.1080/09513590903015544
After three months of taking 2000 mg of myo-inositol per day, 27 women were completely clear, 17 had moderate acne, and 6 still has severe acne.
There are tons of studies on myo- and d-chiro-inositol and how they affect various health problems. I won’t bore you by go over all of them. I’ll conclude with this snippet from a systemic review of myo-inositol on metabolic health problems.
The most important result of Santamaria and Giordanno et al. studies is the critical reduction in serum insulin and, consequently, insulin resistance (HOMA-IR index), which was about double compared to other insulin-sensitizing substances such as pioglitazone, rosiglita zone, and metformin that are or were, at the moment, the gold standard of therapy for patients with impaired glucose tolerance.
Croze, M. L. & Soulage, C. O. Potential role and therapeutic interests of myo-inositol in metabolic diseases. Biochimie 95,1811–27 (2013). https://www.ncbi.nlm.nih.gov/pubmed/23764390
Let that sink in for a while. This dirt cheap supplement reduced insulin resistance twice as effectively as the currently prescribed drugs.
The same review also recommended that doctors give PCOS patients myo-inositol rather than prescription drugs.
Dosage
The studies commonly used the following doses:
- Myo-inositol: 2 – 4 g/day taken twice a day. So 1 – 2 g in the morning and evening.
- D-chiro-inositol: 0.5 – 1 g/day.
Studies show that both myo- and d-chiro-inositol reduce insulin resistance and hormonal imbalances associated with acne. However, it seems that myo-inositol is better at reducing insulin resistance while d-chiro-inositol works better to reduce androgen hormones.
Indeed, studies suggest that combining both forms works better than supplementing with either alone. Studies on combining the two inositol forms are still rather sparse, but the current data shows that the ratio of 40:1 (myo- : D-chiro-inositol) works the best. One study showed that women taking 550 mg myo- and 13.8 mg D-chiro-inositol got better results than women taking 2000 mg of myo-inositol. However, the combination was delivered in a soft capsule form whereas the myo-inositol was given as powder. Apparently, soft capsules work better and require 66% lower dosage.
So perhaps you can aim for the following combination dose:
- Myo-inositol: 1000 to 1500mg/day
- D-chiro-inositol: 25 to 37.5mg/day
You should never supplement with D-chiro-inositol alone.
As far as I know, Ovasitol is the only supplement that combines myo- and D-chiro in the optimal 40:1 ratio. Alas, it’s a bit expensive ($90 for a 90-day supply).
As an alternative, you can buy both individually. For example, you could try the following:
- Myo-inositol from Jarrow Formulas. Costs $10 for 100 750mg capsules, take 2 per day = $0.2/day.
- D-chiro from Discover Nutrition. 300mg per capsule, so take 1 every 10 days. Costs $28 for 60 caps, or 600 day supply = $0.05/day.
Safety
By all accounts, myo-inositol supplements are safe and well tolerated.
In human, myo-inositol in a daily dose up to 18 g per os for 3 months or 2 g/day for 1 year is safe and well tolerated. Side effects, when present, are mild and mainly gastrointestinal in nature (nausea, flatus and diarrhea).
Croze, M. L. & Soulage, C. O. Potential role and therapeutic interests of myo-inositol in metabolic diseases. Biochimie 95,1811–27 (2013). https://www.ncbi.nlm.nih.gov/pubmed/23764390
Another paper had this to say:
Remarkably, in all the studies analyzed, no side effects were reported at the doses of both 2 and 4 g/day.
Dinicola, S., Chiu, T. T., Unfer, V., Carlomagno, G. & Bizzarri, M. The rationale of the myo-inositol and D-chiro-inositol combined treatment for polycystic ovary syndrome. J Clin Pharmacol 54,1079–92 (2014). https://www.ncbi.nlm.nih.gov/pubmed/25042908
However, there are some concerns that supplementing with high doses of D-chiro-inositol alone could have adverse effects on ovarian function. It seems that taking D-chiro-inositol alone imbalances the tissue concentration of myo- and D-chiro-inositols, and this negatively affects the ovaries. The effects have been shown at doses of 600mg/day and higher.
Therefore, I recommend either supplementing with myo-inositol alone or combination of the two and never with D-chiro-inositol alone.
